Infertility means not having children after one year of regular sexual life without the use of contraception techniques (rx). Infertility is one of the major health care problems in all societies worldwide. The average prevalence of infertility in developed countries is 3.5-16.7% and in developing countries is 6.9-9.3% (rx). The overall average of infertility was reported by 13.2% in Iran (rx). Causes of infertility are numerous such as anatomical, physiological and genetic factors. Many environmental and acquired factors also influence fertility and may lead to infertility. Menstrual and ovulation dysfunction and uterine factors are the most common causes of impairment infertility. The etiology of infertility prevalence and patterns of causes of infertility in different regions are diverse. This discrepancy is due to the existence of differences in environmental conditions associated with reproductive behaviors, such as age at marriage, environmental pollution, smoking, and alcohol abuse, changing in lifestyle and diet (rx).
The World Health Organization[rx] defines infertility as follows[rx]
Infertility is “a disease of the reproductive system defined by the failure to achieve a clinical pregnancy after 12 months or more of regular unprotected sexual intercourse (and there is no other reason, such as breastfeeding or postpartum amenorrhoea). Primary infertility is infertility in a couple who have never had a child. Secondary infertility is a failure to conceive following a previous pregnancy. Infertility may be caused by an infection in the man or woman, but often there is no obvious underlying cause.

Causes of Infertility
- Low sperm count – The man ejaculates a low number of sperm. A sperm count of under 15 million is considered low. Around one-third of couples have difficulty conceiving due to a low sperm count.
- Low sperm mobility (motility) – The sperm cannot “swim” as well as they should to reach the egg.
- Abnormal sperm – The sperm may have an unusual shape, making it harder to move and fertilize an egg.
If the sperm do not have the right shape, or they cannot travel rapidly and accurately towards the egg, conception may be difficult. Up to 2 percent of men are thought to have suboptimal sperm. Abnormal semen may not be able to carry the sperm effectively.
This can result from
- A medical condition – This could be a testicular infection, cancer, or surgery.
- Overheated testicles – Causes include an undescended testicle, a varicocele, or varicose vein in the scrotum, the
- Use of saunas or hot tubs – wearing tight clothes, and working in hot environments.
- Ejaculation disorders – If the ejaculatory ducts are blocked, semen may be ejaculated into the bladder
- Hormonal imbalance – Hypogonadism, for example, can lead to a testosterone deficiency.
Other Causes May Include
- Genetic factors – A man should have an X and Y chromosome. If he has two X chromosomes and one Y chromosome, as in Klinefelter’s syndrome, the testicles will develop abnormally and there will be low testosterone and a low sperm count or no sperm.
- Mumps – If this occurs after puberty, inflammation of the testicles may affect sperm production.
- Hypospadias – The urethral opening is under the penis, instead of its tip. This abnormality is usually surgically corrected in infancy. If the correction is not done, it may be harder for the sperm to get to the female’s cervix. Hypospadias affects about 1 in every 500 newborn boys.
- Cystic fibrosis – This is a chronic disease that results in the creation of sticky mucus. This mucus mainly affects the lungs, but males may also have a missing or obstructed vas deferens. The vas deferens carries sperm from the epididymis to the ejaculatory duct and the urethra.
- Radiation therapy – This can impair sperm production. The severity usually depends on how near to the testicles the radiation was aimed.
- Some diseases – Conditions that are sometimes linked to lower fertility in males are anemia, Cushing’s syndrome, diabetes, and thyroid disease.
Some medications increase the risk of fertility problems in men.
- Sulfasalazine – This anti-inflammatory drug can significantly lower a man’s sperm count. It is often prescribed for Crohn’s disease or rheumatoid arthritis. Sperm count often returns to normal after stopping the medication.
- Anabolic steroids – Popular with bodybuilders and athletes, long-term use can seriously reduce sperm count and mobility.
- Chemotherapy – Some types may significantly reduce sperm count.
- Illegal drugs – Consumption of marijuana and cocaine can lower the sperm count.
- Age – Male fertility starts to fall after 40 years.
- Exposure to chemicals – Pesticides, for example, may increase the risk.
- Excess alcohol consumption – This may lower male fertility. Moderate alcohol consumption has not been shown to lower fertility in most men, but it may affect those who already have a low sperm count.
- Overweight or obesity – This may reduce the chance of conceiving.
- Mental stress – Stress can be a factor, especially if it leads to reduced sexual activity.
Laboratory studies have suggested that long-term acetaminophen use during pregnancy may affect fertility in males by lowering testosterone production. Women are advised not to use the drug for more than one day.
Male Causes
Risk factors that increase the risk include:
Smoking significantly increases your risk of infertility
- Age – The ability to conceive starts to fall around the age of 32 years.
- Smoking – Smoking significantly increases the risk of infertility in both men and women, and it may undermine the effects of fertility treatment. Smoking during pregnancy increases the chance of pregnancy loss. Passive smoking has also been linked to lower fertility.
- Alcohol – Any amount of alcohol consumption can affect the chances of conceiving.
- Being obese or overweight – This can increase the risk of infertility in women as well as men.
- Eating disorders – If an eating disorder leads to serious weight loss, fertility problems may arise.
- Diet – A lack of folic acid, iron, zinc, and vitamin B-12 can affect fertility. Women who are at risk, including those on a vegan diet, should ask the doctor about supplements.
- Exercise – Both too much and too little exercise can lead to fertility problems.
- Sexually transmitted infections (STIs) – Chlamydia can damage the fallopian tubes in a woman and cause inflammation in a man’s scrotum. Some other STIs may also cause infertility.
- Exposure to some chemicals – Some pesticides, herbicides, metals, such as lead, and solvents have been linked to fertility problems in both men and women. A mouse study has suggested that ingredients in some household detergents may reduce fertility.
- Mental stress – This may affect female ovulation and male sperm production and can lead to reduced sexual activity.
Medical Conditions
Some medical conditions can affect fertility.
- Ovulation disorders appear to be the most common cause of infertility in women. Ovulation is the monthly release of an egg. The eggs may never be released or they may only be released in some cycles. Ovulation disorders can be due to:
- Premature ovarian failure – The ovaries stop working before the age of 40 years.
- Polycystic ovary syndrome (PCOS) – The ovaries function abnormally and ovulation may not occur.
- Hyperprolactinemia – If prolactin levels are high, and the woman is not pregnant or breastfeeding, it may affect ovulation and fertility.
- Poor egg quality – Eggs that are damaged or develop genetic abnormalities cannot sustain a pregnancy. The older a woman is, the higher the risk.
- Thyroid problems – An overactive or underactive thyroid gland can lead to a hormonal imbalance.
- Chronic conditions – These include AIDS or cancer.
- Problems in the uterus or fallopian tubes – can prevent the egg from traveling from the ovary to the uterus, or womb. If the egg does not travel, it can be harder to conceive naturally.
Causes include
- Surgery – Pelvic surgery can sometimes cause scarring or damage to the fallopian tubes. Cervical surgery can sometimes cause scarring or shortening of the cervix. The cervix is the neck of the uterus.
- Submucosal fibroids – Benign or non-cancerous tumors occur in the muscular wall of the uterus. They can interfere with implantation or block the fallopian tube, preventing sperm from fertilizing the egg. Large submucosal uterine fibroids may make the uterus’ cavity bigger, increasing the distance the sperm has to travel.
- Endometriosis – Cells that normally occur within the lining of the uterus start growing elsewhere in the body.
- Previous sterilization treatment – In women who have chosen to have their fallopian tubes blocked, the process can be reversed, but the chances of becoming fertile again are not high.
Medications, treatments, and drugs
Some drugs can affect fertility in a woman.
- Non-steroidal anti-inflammatory drugs (NSAIDs): Long-term use of aspirin or ibuprofen may make it harder to conceive.
- Chemotherapy: Some chemotherapy drugs can result in ovarian failure. In some cases, this may be permanent.
- Radiation therapy: If this is aimed near the reproductive organs, it can increase the risk of fertility problems.
- Illegal drugs: Some women who use marijuana or cocaine may have fertility problems.
- Cholesterol – One study has found that high cholesterol levels may have an impact on fertility in women.
Other Causes
Factors that can cause male, as well as female infertility, are
DNA damage
- DNA damage reduces fertility in female oocytes, as caused by smoking,[rx] other xenobiotic DNA damaging agents (such as radiation or chemotherapy)[rx] or accumulation of the oxidative DNA damage 8-hydroxy-deoxyguanosine[rx]
- DNA damage reduces fertility in male sperm, as caused by oxidative DNA damage,[rx] smoking,[rx] other xenobiotic DNA damaging agents (such as drugs or chemotherapy)[rx] or other DNA damaging agents including reactive oxygen species, fever or high testicular temperature.[rx] The damaged DNA related to infertility manifests itself by the increased susceptibility to denaturation inducible by heat or acid [rx] or by the presence of double-strand breaks that can be detected by the TUNEL assay.[rx]
General factors
- Diabetes mellitus,[rx] thyroid disorders,[rx] undiagnosed and untreated coeliac disease,[rx][rx] adrenal disease[rx]
Hypothalamic-pituitary factors
- Hyperprolactinemia
- Hypopituitarism
- The presence of anti-thyroid antibodies is associated with an increased risk of unexplained subfertility with an odds ratio of 1.5 and 95% confidence interval of 1.1–2.0.[rx]
Environmental factors
- Toxins such as glues – volatile organic solvents or silicones, physical agents, chemical dust, and pesticides.[rx][rx] Tobacco smokers are 60% more likely to be infertile than non-smokers.[rx] German scientists have reported that a virus called Adeno-associated virus might have a role in male infertility,[rx] though it is otherwise not harmful.[rx] Other diseases such as chlamydia and gonorrhea can also cause infertility, due to internal scarring (fallopian tube obstruction).[rx][rx]
- Obesity – The obesity epidemic has recently become is a serious issue, particularly in industrialized nations. The rising number of obese individuals may be due in part to an energy-rich diet as well as insufficient physical exercise. In addition to other potential health risks, obesity can have a significant impact on male and female fertility. BMI (body mass index) may be a significant factor in infertility, as an increase in BMI in the male by as little as three units can be associated with infertility. Several studies have demonstrated that an increase in BMI is correlated with a decrease in sperm concentration, a decrease in motility, and an increase in DNA damage in sperm. A relationship also exists between obesity and erectile dysfunction (ED).
- Low weight – Obesity is not the only way in which weight can impact fertility. Men who are underweight tend to have lower sperm concentrations than those who are at a normal BMI. For women, being underweight and having extremely low amounts of body fat are associated with ovarian dysfunction and infertility and they have a higher risk of preterm birth. Eating disorders such as anorexia nervosa are also associated with extremely low BMI. Although relatively uncommon, eating disorders can negatively affect menstruation, fertility, and maternal and fetal well-being.
Females
- The following causes of infertility may only be found in females. For a woman to conceive, certain things have to happen: vaginal intercourse must take place around the time when an egg is released from her ovary; the system that produces eggs has to be working at optimum levels, and her hormones must be balanced.[rx]
- Other factors that can affect a woman’s chances of conceiving include being overweight or underweight,[rx] or her age as female fertility declines after the age of 30.[rx]
- Sometimes it can be a combination of factors, and sometimes a clear cause is never established.
Common causes of infertility of females include
- Ovulation problems (e.g. polycystic ovarian syndrome, PCOS, the leading reason why women present to fertility clinics due to anovulatory infertility.[rx])
- Tubal blockage
- A pelvic inflammatory disease caused by infections like tuberculosis
- Age-related factors
- Uterine problems
- Previous tubal ligation
- Endometriosis
- Advanced maternal age
- Immune infertility
Symptoms of Infertility
In women, changes in the menstrual cycle and ovulation may be a symptom of a disease related to infertility. Symptoms include:
- Abnormal periods – Bleeding is heavier or lighter than usual.
- Irregular periods – The number of days in between each period varies each month.
- No periods – You have never had a period, or periods suddenly stop.
- Painful periods – Back pain, pelvic pain, and cramping may happen.
Sometimes, female infertility is related to a hormone problem. In this case, symptoms can also include
- Skin changes, including more acne
- Changes in sex drive and desire
- Dark hair growth on the lips, chest, and chin
- Loss of hair or thinning hair
- Weight gain
- Milky white discharge from nipples unrelated to breastfeeding
- Pain during sex
- Many other things can lead to infertility in women, and their symptoms vary.
- Painful or irregular periods (menstrual cycle)
- Age (older than 35)
- Endometriosis or pelvic inflammatory disease (diseases of a woman’s reproductive organs)
- Cancer treatment
Infertility Symptoms in Men
- Changes in hair growth
- Changes in sexual desire
- Infections
- A low sperm count (a higher count increases the chance the sperm and egg will meet)
- Problems with your male reproductive organs (such as undescended testicles, enlarged prostate, and varicoceles, or enlarged veins in the skin that surround a man’s testicles)
- Cancer treatment
- Pain, lump, or swelling in the testicles
- Problems with erections and ejaculation
- Small, firm testicles
Diagnosis of Infertility
Medical history of a subfertile couple
Woman
-
Previous contraception and any problems (such as “lost” intrauterine contraceptive device)
-
Previous pregnancies and outcome
-
Medical history (such as pelvic infection, Crohn’s disease)
-
Surgical history (such as ovarian cyst, appendicectomy)
-
Gynecological history (such as cone biopsy, cervical smear history)
-
Current medical illness
-
Drug treatments; prescribed and “recreational”
-
Diet
-
Smoking, alcohol consumption, excessive caffeine intake
-
Galactorrhoea
-
Hirsutism (may be disguised)
-
Menstrual regularity and menorrhagia
-
Dysmenorrhoea
-
Intermenstrual or postcoital bleeding
-
Preovulatory cervical mucus recognition
-
Coital frequency and timing
Man
-
Occupation (exposure to excessive heat or toxin, such as cellulose thinners)
-
Medical history (such as mumps, venereal infections)
-
Surgical history (such as orchidopexy, inguinal hernia repair)
-
Current medical illness
-
Prescribed drug treatments (such as sulfasalazine)
-
Drug misuse (such as anabolic steroids)
-
Smoking, alcohol consumption, excessive caffeine intake
-
Erectile or ejaculatory difficulty
An additional test for women
She will also undergo a gynecologic examination and a number of tests:
- Blood test – This can assess hormone levels and whether a woman is ovulating.
- Hysterosalpingography – Fluid is injected into the woman’s uterus and X-rays are taken to determine whether the fluid travels properly out of the uterus and into the fallopian tubes. If a blockage is present, surgery may be necessary.
- Laparoscopy – A thin, flexible tube with a camera at the end is inserted into the abdomen and pelvis, allowing a doctor to look at the fallopian tubes, uterus, and ovaries. This can reveal signs of endometriosis, scarring, blockages, and some irregularities of the uterus and fallopian tubes.
Other tests include
- ovarian reserve testing, to find out how effective the eggs are after ovulation
- genetic testing, to see if a genetic abnormality is interfering with fertility
- pelvic ultrasound, to produce an image of the uterus, fallopian tubes, and ovaries
- Chlamydia test, which may indicate the need for antibiotic treatment
- thyroid function test, as this may affect the hormonal balance
Ovulation testing
- Various methods of predicting fertility exist, to either aid or avoid pregnancy.
Stretch test
- Cervical mucus, Cervical mucus becomes clear and stretchy during the fertile window, to allow sperm to survive in and travel through it. The consistency of fertile mucous is akin to egg white.
Ovulation prediction kit
Electronic fertility monitors[edit]
- A fertility monitor is an electronic device which may use various methods to assist the user with fertility awareness. A fertility monitor may analyze changes in hormone levels in urine, basal body temperature, the electrical resistance of saliva and vaginal fluids, or a combination of these methods. These devices may assist in pregnancy achievement. However, at the moment there is insufficient evidence available to draw conclusions on the effectiveness of fertility monitoring on live births or pregnancies.[rx]
Cervical position
- The cervix becomes soft, high, open, and wet during the fertile window.
Basal Body Temperature Charting
- Basal body temperature changes during the menstrual cycle. Higher levels of progesterone released during the menstrual cycle cause an abrupt increase in basal body temperature by 0.5 °C to 1 °C at the time of ovulation.[rx] This enables the identification of the fertile window through the use of commercial thermometers. This test can also indicate if there are issues with ovulation.[rx]
Calendar methods
- Because the fertile window arrives at approximately the same time each month, calendar methods can be used to predict ovulation.
Diagnosis of infertility
Anti-Müllerian hormone testing
- Anti-Müllerian hormone tests allow the estimation of ovarian reserve. These give an indication of the likely remaining fertility opportunities a woman may have.
Follicle-stimulating hormone
- Tests for follicle-stimulating hormone establish whether or not a woman will ovulate in any given month. This test is typically carried out on day 3 of the menstrual cycle.
Hysterosalpingography
- Hysterosalpingography involves the inspection of the fallopian tubes and uterus, by the injection of a radiocontrast agent, to ensure the egg can pass down the tube without obstruction, and to identify uterine abnormalities.
Transvaginal ultrasound
- Ultrasound is an important tool in evaluating the structure of the uterus, tubes, and ovaries. Ultrasound can detect uterine abnormalities such as fibroids and polyps, distal fallopian tube occlusion, and ovarian abnormalities including ovarian cysts. Additionally, transvaginal ultrasound affords the opportunity for your physician to assess the relative number of available eggs. This measurement is called the antral follicle count and may correlate with fertility potential.
Laboratory testing
- Depending on the results of the evaluation discussed above, your physician may request specific blood tests. The most common of these tests include measurements of blood levels of certain hormones such as estradiol and FSH, which are related to ovarian function and overall egg numbers; TSH, which assesses thyroid function; and prolactin, a hormone that can affect menstrual function if elevated.
Hysterosalpingogram (HSG)
- This test is essential for evaluating fallopian tubal patency, uterine filling defects such as fibroids and polyps, and scarring of the uterine cavity (Asherman syndrome). Many uterine and tubal abnormalities detected by the HSG can be surgically corrected.
Ovarian ultrasound
- Ultrasound scans of the ovaries may be conducted to establish the development of ovarian follicles. This can be useful particularly in the diagnosis of polycystic ovary syndrome.
Hysteroscopy
- Hysteroscopy is used to diagnose the presence of a number of conditions which may affect fertility, such as uterine fibroids, Asherman’s syndrome, and bicornate uterus. It involves the insertion of an endoscope to produce images of the inside of the uterus.
Laparoscopy
- Laparoscopy is used to examine the interior of the abdomen. It can be used to establish patency of the fallopian tubes and is especially suitable for the diagnosis of endometriosis.
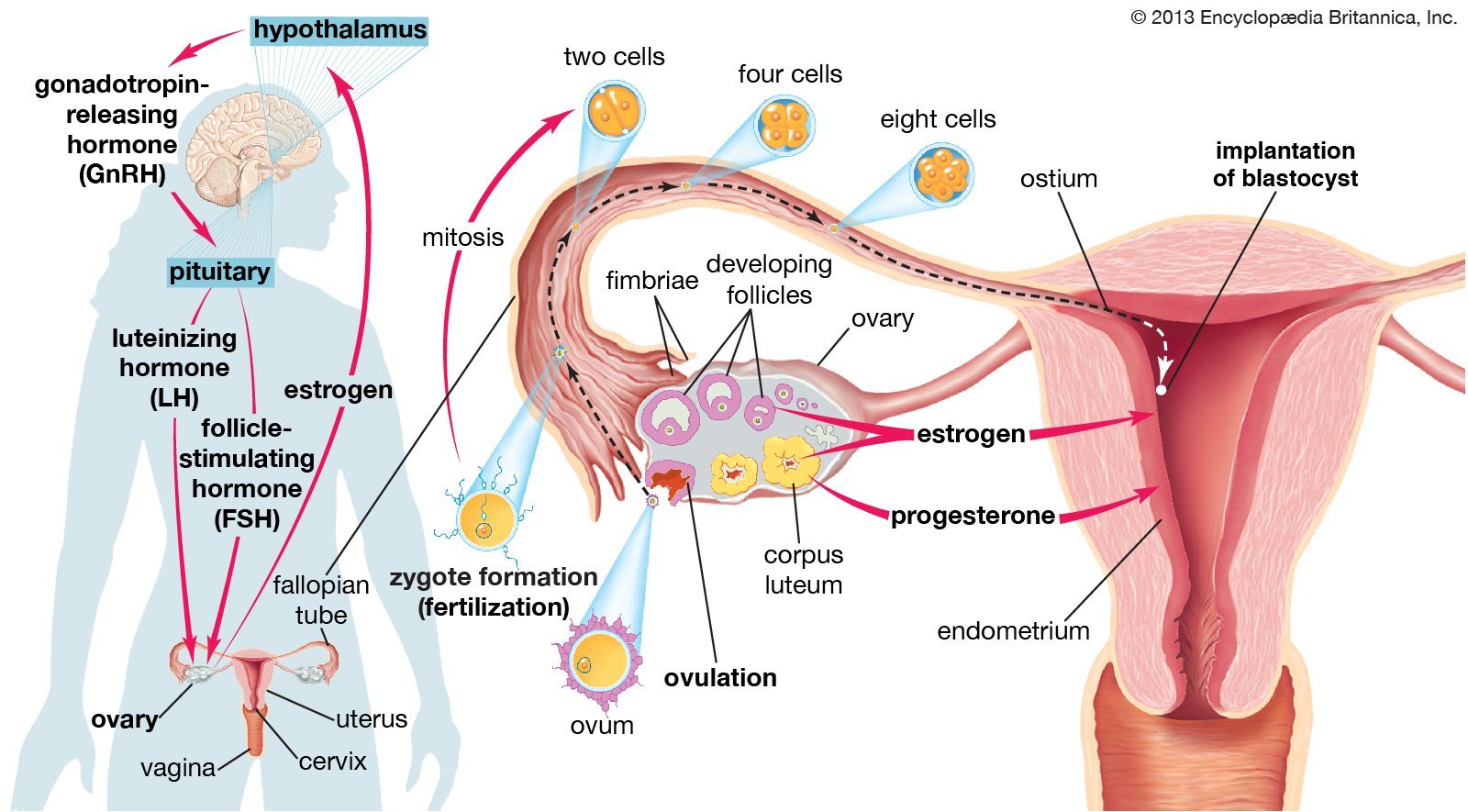
Gonadotropin-Releasing Hormone (GnRH)
- The pulsatile release of GnRH in the hypothalamus stimulates the release of FSH and LH from the anterior pituitary. In men, normal levels of FSH and LH are responsible for the induction of spermatogenesis and maintaining high levels of testicular T (rx).
- Pulsatile administration of GnRH is an effective treatment to replace GnRH deficiency in infertile men with hypogonadotropic hypogonadism (HH) due to a lack of secretion from the hypothalamus (e.g., Kallmann’s syndrome, idiopathic HH). Men with HH have reduced fertility that is usually restored by reestablishing the high intra-testicular T and the FSH stimulation of Sertoli cells (rx).
- The goal of GnRH therapy is to stimulate the release of gonadotropins from the anterior pituitary and subsequent pathways in the HPG (rx). The most effective dose for pulsatile G
Gonadotropins
- The treatment of male infertility in men with pituitary insufficiency (e.g., pituitary adenoma, systemic diseases such as hemochromatosis and sarcoidosis) is based on the use of gonadotropins, therefore spermatogenesis and T production cannot be induced by pulsatile GnRH. Gonadotropins were previously extracted from urine. With the advancement in laboratory technology, human chorionic gonadotropin (rec-hCG), FSH (rec-FSH) and LH (rec-LH) or highly purified urinary gonadotropins are used with superior quality, activity, and performance. There have been no confirmed differences in safety, purity, or clinical efficacy among the various available highly purified or recombinant gonadotropin products (rx).
Dopamine agonist
- For men presenting with infertility and hyperprolactinemia, prolactin-secreting pituitary adenoma (most common functional tumors) should be considered as the underlying cause. Tumors that cause stalk compression and hyperprolactinemia should not be treated with a dopamine agonist.
- Elevated levels of prolactin inhibit the pulsatile secretion of GnRH, men will present with hypogonadism and infertility, and they might also experience headaches or visual field changes secondary to the pituitary tumor compression.
- In this setting, dopamine agonists are indicated for the treatment of infertility and the pituitary tumor. Both bromocriptine and cabergoline have been used in the past. However, there is evidence that cabergoline is more effective than bromocriptine in suppressing prolactin production (rx), and has been shown to normalize prolactin levels in 70% of bromocriptine-resistant patients (rx).
Aromatase inhibitor (AI) therapy
- AI treatment of men with idiopathic OAT or azoospermia is an off-label use of this medication. AIs (anastrozole 1 mg daily, or letrozole 2.5 mg daily) increase T, decrease estrogen levels, and inhibit the peripheral metabolism of T. The intent is to reduce the estrogenic effect on spermatogenesis. High estrogen levels in combination with low T levels have been shown to impair proper spermatogenesis (rx).
- More importantly, elevated levels of estrogen will lead to feedback inhibition of the HPG axis, and the end result is a decrease in the LH necessary for the production T, and FSH to optimize sperm production (rx).
- The activity of aromatase inhibition regardless of patient BMI suggests that aromatase activity in the Leydig cells is responsible for the T to estradiol (E) conversion and impaired semen parameters (rx,rx).
Selective Estrogen Receptor Modulators (SERMs)
- SERMs are a class of compounds that act on the estrogen receptor as agonists or antagonists. Before the introduction of intracytoplasmic sperm injection, SERM’s were one of the few options available for men with idiopathic infertility.
- While SERMs, such as clomiphene citrate (CC), tamoxifen, and toremifene, have been widely used in women for the treatment of breast cancer and osteoporosis, their use in the treatment of male hypogonadism and infertility is currently off-label.
- CC, like other SERMs, inhibits central estrogen feedback (rx) and upregulates the production of LH and FSH, leading to induction of spermatogenesis. Because CC encompasses both strong intrinsic estrogenic and anti-estrogenic properties, there is a concern that the estrogenic effect of clomiphene can potentially have a deleterious effect on spermatogenesis.
- However, studies have shown that, in hypogonadal men, clomiphene can have substantial positive effects on serum T (rx), and can increase pregnancy rates (rx).
Tamoxifen citrate
- Other similar compounds toremifene and raloxifene are non-steroidal estrogen receptor antagonists with a similar mechanism of action as CC at the level of the hypothalamus and pituitary.
- Randomized controlled trials in men with oligospermia or azoospermia examining the efficacy of tamoxifen (20 mg daily) or toremifene and raloxifene (60 mg daily) have reported improvements in semen parameters and pregnancy rates following three months of treatment (rx). However, other studies have shown improvements in the biochemical profile with no effect on semen parameters or fertility outcomes (rx).
Methotrexate (MTX)
- The administration either intramuscularly or in the ectopic sac. MTX is a chemotherapeutic drug given at a dose of 1 mg/kg or based on the surface area calculation of 50 mg/m2. It may be given in single or multiple doses.
- There are currently no randomized controlled trials comparing medical treatment versus salpingectomy. Appropriate patient selection is the crux of successful treatment with MTX. β-hCG levels, size of the ectopic mass, and the presence or absence of yolk sac on ultrasound determine the success of medical therapy.
Metformin
- For assisted reproduction cycles, metformin use prior to or during ovarian stimulation with gonadotropins in IVF/ICSI cycles is also not associated with better clinical pregnancy or live birth rates; however, metformin may reduce the risk of OHSS [rx] and miscarriage and improve the implantation rate because metformin may act directly on the endometrium [rx] and promote better reproductive outcomes (data not confirmed) in women with PCOS [rx]. However, as previously mentioned, the use of a GnRH antagonist combined with ovarian stimulation with gonadotropins in women with PCOS and the induction of final ovarian maturation with a GnRH agonist with subsequent embryo cryopreservation are more effective strategies to prevent OHSS regardless of metformin use [rx]. Thus, the routine use of metformin in cycles of ovarian stimulation for IVF in women with PCOS is not recommended except in the presence of a disorder in glucose metabolism [rx].
Aromatase inhibitors
- Although aromatase inhibitors have been used in women with PCOS as an alternative method to avoid the anti-estrogenic effect of CC on the endometrium, these compounds are not typically used in clinical practice to treat infertility in these patients. Their mechanism of action is based on reducing the peripheral conversion of androgens to estrogens in ovarian granulosa cells by blocking aromatase. Consequently, a decrease in estrogen serum levels and in its negative feedback in the hypothalamus and pituitary gland is noted, resulting in increased endogenous gonadotropin release [rx].
Counseling
- Fertility clinics should address the psycho-social and emotional needs of infertile couples as well as their medical needs. The content of counseling may differ depending on the concerned couple and the existing treatment options. It usually involves treatment implication counseling, emotional support counseling, and therapeutic counseling [rx,rx].
[stextbox id=’info’]
| Substance | Administration | Dosage and frequency | Current availability |
|---|---|---|---|
|
Subcutaneous infusion pump | 25-200 ng/kg per pulse every 2 hours | Only in specialty centers or part of clinical trials |
|
Subcutaneous/intramuscular | 1,500-3,000 IU 2 times/week |
Available, FDA approved for the treatment of infertility due to gonadotropin deficiency |
|
Subcutaneous/intramuscular | 75 IU 2-3 times/week | Available, FDA approved for the treatment of infertility due to gonadotropin deficiency |
|
Subcutaneous/intramuscular | 100-150 IU 2-3 times/week | Available, FDA approved for the treatment of infertility due to gonadotropin deficiency |
|
Oral | Cabergoline (0.5-1 mg twice weekly), bromocriptine (2.5-5.0 mg twice weekly) |
FDA approval for treatment of hyperprolactinemia |
A study headed by Hayashi, Miyata, and Yamada investigated the effects of antibiotics, antidepressants, antiepileptics, β stimulators, H1 and H2 receptor antagonists, mast cell blockers, and sulfonylurea compounds (n = 201) [rx]. Male participants were divided so one group had medication switched or stopped and the other served as the control.
[/stextbox]
- Marijuana – is one of the most commonly used drugs around the world [rx], and it acts both centrally and peripherally to cause abnormal reproductive function. Marijuana contains cannabinoids that bind to receptors located on reproductive structures such as the uterus or the ductus deferens. In males, cannabinoids have been reported to reduce testosterone released from Leydig cells, modulate apoptosis of Sertoli cells, decrease spermatogenesis, decrease sperm motility, decrease sperm capacitation and decrease acrosome reaction [rx].
- Cocaine – a stimulant for both peripheral and central nervous systems that causes vasoconstriction and anesthetic effects. It is thought to prevent the reuptake of neurotransmitters [rx], possibly affecting behavior and mood. Long term users of cocaine claim that it can decrease sexual stimulation; men found it harder to achieve and maintain erection and to ejaculate [rx]. Cocaine has been demonstrated to adversely affect spermatogenesis, which may be due to serum increases in prolactin, as well as serum decreases in total and free testosterone [rx,rx]. Peugh and Belenko suggest that the effects of cocaine in men depend on the dosage, duration of usage, and interactions with other drugs [rx]. While less is known about cocaine’s effects on females, impaired ovarian responsiveness to gonadotropins and placental abruption have both been reported [rx–rx].
- Opiates – comprise another large group of illicit drugs. Opiates, such as methadone and heroin, are depressants that cause both sedation and decreased pain perception by influencing neurotransmitters [rx]. In men taking heroin, the sexual function became abnormal and remained so even after cessation [rx]. Sperm parameters, most noticeably motility, also decrease with the use of heroin and methadone [rx,rx]. In women, placental abruption with the use of heroin may also be a cause of infertility [rx].
- Antioxidant – Increased rates of infertility have been found in men with the seminal fluid containing high levels of reactive oxygen species (ROS) (rx). These ROS are associated with sperm dysfunction, germ cell DNA damage with the possibility of impaired fertility, but the exact mechanism is not completely understood. These associations have led clinicians to treat infertile men with antioxidant supplements. A variety of clinical trials have suggested that the use of antioxidant supplements have a slight benefit in improving sperm function and DNA integrity. However, most of these studies are not randomized controlled trials, and to date, there are no convincing trials that have demonstrated a significantly higher unassisted pregnancy rate after treating men with antioxidant therapy (rx).
Assisted Conception
The following methods are currently available for assisted conception.
- Intrauterine insemination (IUI) – At the time of ovulation, a fine catheter is inserted through the cervix into the uterus to place a sperm sample directly into the uterus. The sperm is washed in a fluid and the best specimens are selected. The woman may be given a low dose of ovary stimulating hormones. IUI is more commonly done when the man has a low sperm count, decreased sperm motility, or when infertility does not have an identifiable cause. It can also help if a man has severe erectile dysfunction.
- In-vitro fertilization (IVF) – Sperm are placed with unfertilized eggs in a petri dish, where fertilization can take place. The embryo is then placed in the uterus to begin a pregnancy. Sometimes the embryo is frozen for future use.
- Intracytoplasmic sperm injection (ICSI) – A single sperm is injected into an egg to achieve fertilization during an IVF procedure. The likelihood of fertilization improves significantly for men with low sperm concentrations.
- Sperm or egg donation – If necessary, sperm or eggs can be received from a donor. Fertility treatment with donor eggs is usually done using IVF.
- Assisted hatching – The embryologist opens a small hole in the outer membrane of the embryo, known as the zona pellucid. The opening improves the ability of the embryo to implant into the uterine lining. This improves the chances that the embryo will implant at, or attach to, the wall of the uterus. This may be used if IVF has not been effective, if there has been poor embryo growth rate, and if the woman is older. In some women, and especially with age, the membrane becomes harder. This can make it difficult for the embryo to implant.
- Electric or vibratory stimulation to achieve ejaculation – Ejaculation is achieved with electric or vibratory stimulation. This can help a man who cannot ejaculate normally, for example, because of a spinal cord injury.
- Surgical sperm aspiration – The sperm is removed from part of the male reproductive tract, such as the vas deferens, testicle, or epididymis.
Surgical Treatment
- Surgery’s aim is to remove macroscopic endometriosis implants and restore normal pelvic anatomy. However, surgery may not be able to completely restore pelvic anatomy or to stop the inflammatory process. Hence, it is important to weigh up the benefits versus harm to the surgical procedure. Laparoscopy is preferred to laparotomy because of the advantages of minimal tissue damage, or magnification, faster recovery, and shorter hospital stay (rx).
Is there a benefit of surgical treatment of stage I–II of endometriosis and successful pregnancy rate?
- Several studies demonstrated that, in infertile women with endometriosis stage I/II of the American Fertility Society/American Society for Reproductive Medicine (AFS/ASRM), clinicians should perform operative laparoscopy (excision or ablation of endometriosis lesions) including adhesiolysis, rather than performing diagnostic laparoscopy only, since there is a positive effect in regards to living birth and ongoing pregnancy at 20 weeks of amenorrhea (rx, rx).
- According to ESHRE guidelines, and concerning the management of women with stage I–II of endometriosis, clinicians may consider CO2 laser vaporization of endometriosis, instead of monopolar electrocoagulation, since laser vaporization is associated with higher cumulative spontaneous pregnancy rates (rx).
Is there a benefit of surgical treatment of stage III-IV of endometriosis and successful pregnancy rate?
- There is no randomized controlled trial or meta-analysis to assess whether surgery is positively effective or not on pregnancy rates in moderate to severe endometriosis. The lack of randomized trials or meta-analysis is not due to lack of research effort but to the unethical aspect of such studies that is to do nothing to a patient with stage III or IV endometriosis who is already under anesthesia could be ethically unacceptable.
How should we behave with ovarian endometrioma in case of infertility?
- According to the ESHRE Guideline (rx) in infertile women with ovarian endometrioma of >3 cm in size, surgeons should perform excision of endometrioma capsule instead of ablative surgery that is drainage and electrocoagulation of the endometrioma wall since it increases the spontaneous postoperative pregnancy rate.
- Excision of endometriomas involves the opening of the cyst (using scissors or electrosurgical or laser energy). After identifying the plane of cleavage between the cyst wall and ovarian tissue, the cyst wall is then excised or “stripped away” by applying opposite bimanual traction and counter actin with two grasping forceps. The ovarian edges could be sutured or inverted by a light application of bipolar coagulation or kept as they are. Ablative surgery also involves the opening and drainage or fenestration (making a window in the wall of the cyst) of the endometrioma, followed by the destruction of the cyst wall using either electrosurgical current, cutting or coagulating current or a form of laser energy.
Is there any association between endometrioma and the risk of ovarian cancer?
- The ESHRE’s GDG concluded that there is no evidence that endometriosis causes cancer, though some cancers are slightly more common in women with endometriosis such as non-Hodgkin’s lymphoma and ovarian cancer (rx).
- A very large study (rx) showed a higher risk of histological subtypes of ovarian cancer in the case of endometriosis. Self-reported endometriosis was associated with a significantly increased risk of clear cell ovarian cancer, low-grade serous ovarian cancer, and endometrial invasive ovarian cancer. Clinicians should be aware of this increased risk and future efforts should be focused on understanding the mechanisms that might lead to malignant transformation of endometriosis so as to help identify subsets of women at increased risk of ovarian cancer.
[stextbox id=’custom’]
Medications and their respective effects on both male and female reproductive function
| Medication | Effect on reproductive function |
|---|---|
| Anabolic Steroids
|
Impairment of spermatogenesis (up to one-year recovery); may cause hypogonadism through the pituitary-gonadal axis
|
| Reversible
|
|
| Antiandrogens:
|
Impairment of spermatogenesis; erectile dysfunction
|
| Cyproterone acetate, danazol, finasteride, ketoconazole, spironolactone
|
Reversible
|
| Antibiotics:
|
Impairment of spermatogenesis
|
| Ampicillin, cephalothin, cotrimoxazole, gentamycin, neomycin, nitrofurantoin, Penicillin G, spiramycin
|
Reversible
|
| Antibiotics:
|
Impairment of sperm motility
|
| Cotrimoxazole, dicloxacillin, erythromycin, lincomycin, neomycin, nitrofurantoin, quinolones, tetracycline, tylosin
|
|
| Reversible
|
|
| Antiepileptics:
|
Impairment of sperm motility
|
| Phenytoin
|
Reversible
|
| Antihypertensives:
|
Fertilization failure
|
| Calcium channel blockers (nifedipine)
|
|
| Antihypertensives:
|
Erectile dysfunction
|
| Alpha agonists (clonidine), alpha-blockers (prazosin), beta-blockers, hydralazine, methyldopa, thiazide diuretics
|
|
| Anti-inflammatory 5-ASA and derivatives:
|
Impairment of spermatogenesis and sperm motility
|
| Mesalazine, sulfasalazine
|
Reversible
|
| Antimalarials:
|
Impairment of sperm motility
|
| Quinine and its derivatives
|
Reversible
|
| Antimetabolites ⁄ Antimitotics:
|
The arrest of spermatogenesis; azoospermia
|
| Irreversible
|
|
| Colchicines, cyclophosphamide
|
|
| Anti-oestrogens
|
Impairment of endometrial development
|
| Clomiphene citrate
|
reversible
|
| Anti-progestins:
|
Impairment of both implantation and tubal function
|
| Emergency contraceptive pills, progesterone-only pills
|
|
| Antipsychotics:
|
Increase prolactin concentrations that can lead to sexual dysfunction
|
| Alpha-blockers, phenothiazine, antidepressants (particularly SSRIs)
|
|
| Antipsychotics:
|
Impairment of spermatogenesis and sperm motility
|
| Butyrophenones
|
Reversible
|
| Antischistozomal:
|
Impairment of spermatogenesis and sperm motility
|
| Niridazole
|
Reversible
|
| Corticosteroids
|
Impairment of sperm concentration and motility
|
| Reversible
|
|
| Exogenous testosterone, GnRH analogs
|
Impairment of spermatogenesis
|
| Reversible
|
|
| H2 blockers:
|
Increase prolactin concentrations that can lead to impairment of luteal function, loss of libido, and erectile dysfunction
|
| Cimetidine, ranitidine
|
|
| Local anesthetics, halothane
|
Impair sperm motility
|
| Metoclopramide
|
Erectile dysfunction
|
| Methadone
|
Suppress spermatogenesis and sperm motility
|
| Non-steroidal anti-inflammatory drugs, Cox-2 inhibitors | Impairment of follicle rupture, ovulation, and tubal function
|
| Reversible |
[/stextbox]
Prevention
Acquired female infertility may be prevented through identified interventions:
- Maintaining a healthy lifestyle – Excessive exercise, consumption of caffeine and alcohol, and smoking have all been associated with decreased fertility. Eating a well-balanced, nutritious diet, with plenty of fresh fruits and vegetables, and maintaining a normal weight, on the other hand, have been associated with better fertility prospects.
- Treating or preventing existing diseases – Identifying and controlling chronic diseases such as diabetes and hypothyroidism increases fertility prospects. The lifelong practice of safer sex reduces the likelihood that sexually transmitted diseases will impair fertility; obtaining prompt treatment for sexually transmitted diseases reduces the likelihood that such infections will do significant damage. Regular physical examinations (including pap smears) help detect early signs of infections or abnormalities.
- Not delaying parenthood – Fertility does not ultimately cease before menopause, but it starts declining after age 27 and drops at a somewhat greater rate after age 35.[rx] Women whose biological mothers had unusual or abnormal issues related to conceiving may be at particular risk for some conditions, such as premature menopause, that can be mitigated by not delaying parenthood.
- Egg freezing – A woman can freeze her eggs preserve her fertility. By using egg freezing while in the peak reproductive years, a woman’s oocytes are cryogenically frozen and ready for her use later in life, reducing her chances of female infertility.[rx]
Some strategies suggested or proposed for avoiding male infertility include the following:
- Avoiding smoking[rx] as it damages sperm DNA
- Avoiding heavy marijuana and alcohol use.[rx]
- Avoiding excessive heat to the testes.[rx]
- Maintaining optimal frequency of coital activity: sperm counts can be depressed by daily coital activity[rx] and sperm motility may be depressed by coital activity that takes place too infrequently (abstinence 10–14 days or more).[rx]
- Wearing a protective cup and jockstrap to protect the testicles, in any sport such as baseball, football, cricket, lacrosse, hockey, softball, paintball, rodeo, motocross, wrestling, soccer, karate or other martial arts or any sport where a ball, foot, arm, knee or bat can come into contact with the groin.
- Diet – Healthy diets (i.e. the Mediterranean diet) rich in such nutrients as omega-3 fatty acids, some antioxidants and vitamins, and low in saturated fatty acids (SFAs) and trans-fatty acids (TFAs) are inversely associated with low semen quality parameters. In terms of food groups, fish, shellfish and seafood, poultry, cereals, vegetables and fruits, and low-fat dairy products have been positively related to sperm quality.
Glossary
[stextbox id=’info’]
| Anovulation | is the failure to ovulate (expel a mature oocyte) owing to dysfunction of the ovary or suppression by drug treatment. Anovulation is a common cause of female infertility. Most often, women who do not ovulate also do not menstruate (amenorrhoea). |
| Assisted hatching procedure | Assisted hatching is a process to breach the zona pellucida of an embryo, by either laser or chemical processes, potentially to improve its implantation potential. |
| Delayed in vitro fertilization | In vitro fertilization treatment after 6 months of being assessed in an infertility clinic after at least 12 months of infertility. |
| Endometriosis | is a progressive disease that occurs when the endometrial tissue lining the uterus grows outside the uterus and attaches to the ovaries, fallopian tubes, or other organs in the abdominal cavity. Symptoms include painful menstrual periods, abnormal menstrual bleeding, and pain during or after sexual intercourse. |
| Gonadotrophin priming of oocytes | This is the in vitro maturation of oocytes using gonadotrophins (hormones stimulate and control reproductive activity) from the germinal vesicle (early) stage of development to the metaphase II (mature) stage. |
| High-quality evidence | Further research is very unlikely to change our confidence in the estimate of effect. |
| Hydrosalpinges | is the abnormal distension of one or both fallopian tubes owing to fluid build-up, usually because of inflammation. |
| Hydrotubation | Flushing of the fallopian tubes through the cervix and uterine cavity to remove surgical debris and reduce the incidence of tubal occlusion. |
| Immediate in vitro fertilization | In vitro fertilization treatment within 6 months of being assessed in an infertility clinic after at least 12 months of infertility. |
| In vitro fertilization | (IVF) is a technique where female oocytes (eggs) are fertilized with sperm from a male partner outside the body in a fluid medium in the laboratory. Embryos are transferred later to the uterus using a special catheter. |
| Long agonist protocol | is the most widely used protocol for an in vitro fertilization (IVF) cycle, which involves starting the gonadotrophin-releasing hormone (GnRH) agonist usually on the 21st day of the menstrual cycle. Ovarian stimulation with follicle-stimulating hormone (FSH) then starts a couple of days after the onset of menstruation. |
| Low-quality evidence | Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. |
| Microsurgery | Surgery without dedicated optical magnification. |
| Microsurgery | Surgery involving optical magnification to allow the use of much finer instruments and suture material in addition to a non-touch technique, with the aim of minimising tissue handling and damage. |
| Moderate-quality evidence | Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. |
| Ovarian hyperstimulation syndrome (OHSS) | can occur in mild, moderate, and severe forms. Mild ovarian hyperstimulation syndrome is characterized by fluid accumulation, as shown by weight gain, abdominal distension, and discomfort. Moderate ovarian hyperstimulation syndrome is associated with nausea and vomiting, ovarian enlargement, abdominal distension, discomfort, and dyspnoea. Severe ovarian hyperstimulation syndrome is a life-threatening condition, in which there is a contraction of the intravascular volume, tense ascites, pleural and pericardial effusions, severe haemoconcentration, and the development of hepatorenal failure. Deaths have occurred, caused usually by cerebrovascular thrombosis, renal failure, or cardiac tamponade. |
| Ovulation disorders | are defined by the failure of an ovum to be expelled owing to a malfunction in the ovary. Ovulation disorders are a major cause of infertility and can often be corrected with medication. Ovulation disorders often result in infrequent menstruation (oligomenorrhoea). |
| Pituitary downregulation (long protocol) | This is the process by which the release of gonadotrophins from the pituitary gland is stopped after repeated administration of gonadotrophin-releasing hormone (GnRH) analogs; this, in turn, controls reproductive function. |
| Polycystic ovary syndrome (PCOS) | results from an accumulation of incompletely developed follicles in the ovaries owing to chronic anovulation. PCOS is characterized by irregular or absent menstrual cycles, multiple small cysts on the ovaries (polycystic ovaries), mild hirsutism, and infertility. Many women also have increased insulin resistance. |
| Pulsatile gonadotrophin-releasing hormone | is a hormone produced and released by the hypothalamus at intervals (pulses). The pulsatile gonadotrophin-releasing hormone controls the production and release of gonadotrophins from the pituitary gland, which in turn controls reproductive function. |
| Salpingography | is a technique used to diagnose blockages in the fallopian tubes? It involves the radiographic imaging of the fallopian tubes after the injection of radio-opaque contrast medium (dye) through the cervix to the uterine cavity. If the fallopian tubes are open the dye flows into the tubes and then spills out to the abdominal cavity. This is documented in a series of x-ray images during the procedure. If tubes are blocked from the proximal end, a very narrow catheter is introduced under radiographic imaging (selective salpingography and tubal catheterization) to remove the obstruction if possible. |
| Second look laparoscopy | Laparoscopy performed sometime after tubal surgery (either open or laparoscopic) with the aim of dividing adhesions relating to the initial procedure. |
| Tubal flushing | involves injecting an oil or water-soluble contrast medium into the fallopian tubes to flush out any blockages in the tubes. Flushing out any tubal “plugs” that may be causing proximal tubal occlusion using oil or water-soluble media may have a fertility-enhancing effect. |
| Tubal infertility | is the inability to conceive owing to a blockage in one or both fallopian tubes and is a common cause of infertility. The tubal blockages are usually caused either by pelvic infection, such as pelvic inflammatory disease (PID) or endometriosis. Blockages may also be caused by scar tissue that forms after pelvic surgery. |
| Tubal surgery | techniques are used to restore the patency of the fallopian tubes in women with tubal infertility as an alternative to in vitro fertilization. Surgery may either be open microsurgery or laparoscopic microsurgery. |
| Very low-quality evidence | Any estimate of effect is very uncertain. |
[/stextbox]
References
[bg_collapse view=”button-orange” color=”#4a4949″ expand_text=”Show More” collapse_text=”Show Less” ]
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3217752/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1988991/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4637117/
- https://academic.oup.com/humrep/article/29/5/1067/2913997
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4708300/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3043157/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4642490/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4286960/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3493829/
- https://en.wikipedia.org/wiki/Infertility
- https://en.wikipedia.org/wiki/Female_infertility
- https://en.wikipedia.org/wiki/Male_infertility
- https://familydoctor.org/condition/infertility/
- http://obgyn.ucla.edu/infertility
- https://www.mayoclinic.org/diseases-conditions/infertility/symptoms-causes/syc-20354317
- https://www.nhs.uk/conditions/infertility/
- https://www.webmd.com/infertility-and-reproduction/guide/understanding-infertility-
- https://www.cdc.gov/reproductivehealth/infertility/index.htm
[/bg_collapse]

Visitor Rating: 5 Stars
Visitor Rating: 5 Stars