Shoulder impingement syndrome is a common condition affecting the shoulder often seen in aging adults. This condition is closely related to shoulder bursitis and rotator cuff tendonitis. These conditions may occur alone or in combination. It is a clinical syndrome which occurs when the tendons of the rotator cuff muscles become irritated and inflamed as they pass through the subacromial space, the passage beneath the acromion. This can result in pain, weakness, and loss of movement at the shoulder.
Another’s Name of Shoulder Impingement
Shoulder impingement syndrome,subacromial impingement ,painful arc syndrome, supraspinatus syndrome,swimmer’s shoulder, thrower’s shoulder,
Anatomy of Shoulder Impingement
There are basically 5 structures that can cause compression
- Supraspinatus muscle
- Infraspinatus muscle
- Calcification
- Shoulder bursitis
- Head of the humerus
2. Acromion
- 3 ossification centers unite to form the acromion meta-acromion (base)
- Meso-acromion (mid)
- Pre-acromion (tip)
- failure of the ossification centers to fuse results in an os acromiale
3. Associated conditions
- Hook-shaped acromion
- Os acromiale
- Posterior capsular contracture
- Scapular dyskinesia
- Tuberosity fracture malunion
- Instability
3. The rotator cuff is a common source of pain in the shoulder. Pain can be the result of
- Tendinitis – The rotator cuff tendons can be irritated or damaged.
- Bursitis – The bursa can become inflamed and swell with more fluid causing pain.
- Impingement – When you raise your arm to shoulder height, the space between the acromion and rotator cuff narrows. The acromion can rub against (or “impinge” on) the tendon and the bursa, causing irritation and pain.
Causes of Shoulder Impingement
There are several causes to shoulder impingement syndrome including:
- Repetitive overhead movements, such as golfing, throwing, racquet sports, and swimming, or frequent overhead reaching or lifting.
- Injury, such as a fall, where the shoulder gets compressed.
- Bony abnormalities of the acromion, which narrow the subacromial space.
- Osteoarthritis in the shoulder region.
- Poor rotator cuff and shoulder blade muscle strength, causing the humeral head to move abnormally.
- Thickening of the bursa.
- Thickening of the ligaments in the area.
- The tightness of the soft tissue around the shoulder joint called the joint capsule.
Symptoms of Shoulder Impingement
These symptoms may include
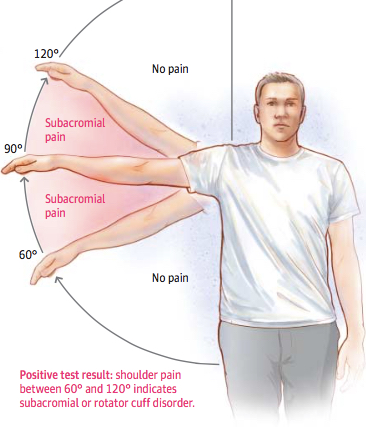
- An arc of shoulder pain approximately when your arm is at shoulder height and/or when your arm is overhead.
- Shoulder pain that can extend from the top of the shoulder to the elbow.
- Pain when lying on the sore shoulder.
- Shoulder pain at rest as your condition deteriorates.
- Muscle weakness or pain when attempting to reach or lift.
- Pain when putting your hand behind your back or head.
- Pain reaching for the seat-belt.
- Minor pain that is present both with activity and at rest
- Pain radiating from the front of the shoulder to the side of the arm
- Sudden pain with lifting and reaching movements
- Athletes in overhead sports may have pain when throwing or serving a tennis ball
As the problem progresses, the symptoms increase:
- Pain at night
- Loss of strength and motion
- Difficulty doing activities that place the arm behind the back, such as buttoning or zippering
Diagnosis of Shoulder Impingement
Physical exam
- Strength – Usually normal
- Impingement tests (see complete physical exam of the shoulder) positive Neer impingement sign Positive if passive forward flexion >90° causes pain
3. Positive Neer impingement test
- If a subacromial injection relieves pain associated with passive forward flexion >90°
- Positive Hawkins test
- positive if internal rotation and passive forward flexion to 90° causes pain
- Jobe test
- pain with resisted pronation and forward flexion to 90° indicates supraspinatus pathology
- Painful Arc Test
- Yocum Test
- positive if pain reproduced with elbow elevation while ipsilateral hand placed on contralateral shoulder
- sensitive but nonspecific
- Internal Impingement test
- positive if pain is elicited with the abduction and external rotation of the shoulder
{kind=link}
- Take medical history, with emphasis on pain, sleep disturbance, loss of function and treatments.
- Perform a physical examination, documenting the range of motion, strength and shoulder impingement signs.
Imaging tests
In order to understand the state of the rotator cuff tendons, bursal inflammation or bone spur formation, imaging scans are required:
- X-rays – do not show tendons but may show changes in the shoulder blade shape (spur, increased curvature or tilt) that may narrow the tunnel over the rotator cuff tendons. X-rays also exclude arthritis of the ball and socket or collar bone/shoulder blade (AC) joint that can also cause shoulder pain.
- Ultrasound – can visualize the bursa and rotator cuff tendons, compare both shoulders and examine the tendons for impingement with arm elevation.
- MRI – can create detailed images of both bone and soft tissues. An MRI can show bursitis, tendon thickening or tear and tunnel narrowing due to bony or ligament prominence. MRI scans require laying down in a tunnel and may not be tolerated by people with claustrophobia. MRI scan showing pinching and damage to the tendon under the narrow tunnel.
Treatment of Shoulder Impingement
- Rest – Use pain as your guide. You are only aggravating the condition if you continue your activity while experiencing pain. In very bad cases, you should refrain from using your arm for all daily activities (lifting briefcase, opening doors).
- Ice – In the early, painful stage, apply ice (frozen peas) to your shoulder twice a day for 15 minutes. Always apply ice for 15 minutes after any activity using your arm.
- Range – When the use of your arm is limited, range exercises must be done twice daily. Bend at the waist and let your arm hang down. Then make large circles with your arm. These pendulum exercises will prevent your shoulder from becoming stiff.
Medication
Your doctor may prescribe anti-inflammation pills. These could form a very important part of the treatment.
- Analgesics – Prescription-strength drugs that relieve pain but not inflammation.
- Antidepressants – A Drug that blocks pain messages from your brain and boosts the effects of exorphins (your body’s natural painkillers).
- Medication – Common pain remedies such as aspirin, acetaminophen, ibuprofen, and naproxen can offer short-term relief. All are available in low doses without a prescription. Other medications, including muscle relaxants and anti-seizure medications, treat aspects of spinal stenoses, such as muscle spasms and damaged nerves.
- Corticosteroid injections – Your doctor will inject a steroid such as prednisone into your back or neck. Steroids make the inflammation go down. However, because of side effects, they are used sparingly.
- Manual Therapy – Your physical therapist may use manual techniques, such as gentle joint movements, soft-tissue massage, and shoulder stretches to get your shoulder moving properly so that the tendons and bursa avoid impingement.
- Range-of-Motion Exercises – You will learn exercises and stretches to help your shoulder and shoulder blade move properly, so you can return to reaching and lifting without pain.
- Mobility and stretching – Stretches can be done on a daily basis assuming there is no pain. Stretching must be done regularly and continued throughout the rehabilitation process. Below are some important stretches would be performed in order to encourage a full range of motion and improved posture.
Chest stretch
- Place one forearm arm against a fixed point such as a doorframe or corner of a wall.
- Gently lean forward and turn away from it to stretch the chest muscles.
- Again, hold the position for 20 to 30 seconds and repeat 3 times. The athlete should feel a gentle stretch in the front of the shoulder but not pain.
Supraspinatus Stretch
- Place the hand on the lower back and use the other hand to pull the elbow forwards.
- Keep your hand on your lower back.
- You should feel a gentle stretch at the back of the shoulder.
- Hold for 20 to 30 seconds and repeat 5 times assuming there is no pain. If it is painful then discontinue.
Anterior shoulder stretch
- Grasp something above you such as a doorframe (or something similar if not tall enough).
- Move forwards leaving the arm behind to stretch the front of the shoulder and chest muscles.
- Hold the position for 20 to 30 seconds and repeat 3 times.
- The athlete should feel a gentle stretch in the front of the shoulder but not pain.
Posterior shoulder stretch
- Place one arm across the front and pull it in tight with the other.
- The athlete should feel a gentle stretch at the back of the shoulder.
- Again, hold the position for 20 to 30 seconds and repeat 3 times. The athlete should feel a gentle stretch in the back of the shoulder but not pain.
- Stretching should be done as soon as pain will allow and maintained throughout the rehabilitation process and beyond. Little and often is generally better than a big effort for a few days and then forgetting it as soon as the athlete feels the injury has settled down.
Strengthening exercises
- The strengthening exercises below are aimed at strengthening the rotator cuff muscles which are involved in stabilizing the shoulder joint. There is also an emphasis on the upper back muscles such as the Rhomboids and Serratus Anterior which improve posture.
- Always make sure any strengthening exercises are pain-free. If there is any pain, stop immediately.
Strengthening Exercises
- Your physical therapist will determine which strengthening exercises are right for you, depending on your specific condition. Often with shoulder impingement syndrome, the head of the humerus tends to drift forward and upward due to the rotator-cuff muscles becoming weak. Strengthening the rotator-cuff and scapular muscles helps position the head of the humerus bone down and back to ease the impingement. You may also perform resistance training exercises to strengthen your weaker muscles. You will receive a home-exercise program to continue your strengthening long after you have completed your formal physical therapy.
External rotation lying
- The athlete lies on their side with the arm to be worked on top.
- The upper arm should be resting on your side and the elbow bent so that the hand points towards the floor.
- Rotate the shoulder so that the hand moves up, towards the ceiling as far as possible.
- Slowly return to the starting position.
- Start with a light weight of around 2kg.
- Aim for 10 to 20 repetitions.
- This exercise may be performed daily.
This exercise can also be performed in a standing position with resistance band.
Internal rotation lying
- Lay on your side with the arm to be worked on the bottom. Start with the forearm parallel to the floor.
- Rotate the shoulder so that the forearm moves towards the stomach and hand points upwards.
- Slowly lower the weight back to the start. Start with a light weight of around 2-3kg.
- Aim for 10-20 repetitions initially. This exercise should be performed daily.
This exercise can also be performed in a standing position with resistance band.
External rotation in abduction
- The athlete stands with the arm abducted (raised to the side) to 90 degrees – so the arm is parallel to the floor.
- If it is easier the elbow can be rested on a chair or bench (in a seated position).
- The elbow should also be bent to 90 degrees.
- Using the elbow as a fixed point, rotate the shoulder so that the hand points to the ceiling.
- Slowly return to the starting position.
- Start with a 2-3kg dumbbell, or use a cable pulley machine or resistance band.
- Aim for 10-20 repetition initially.
It is also important in all shoulder rehabilitation to strengthen the muscles of the shoulder girdle in order to maintain correct shoulder biomechanics. The shoulder girdle consists of the shoulder blade (scapular) and the collar bone (clavicle). The following exercises are designed to strengthen the shoulder girdle.
Retraction
- The athlete aims to pull the shoulder back, whilst keeping the arm straight and the head still.
- The only thing to move when doing this exercise should be the shoulder.
- Aim to build up gradually (without a weight at first) from 3 sets of 10 repetitions to 3 sets of 30.
- Once 3 sets of 30 are reached with no adverse affects, then the weight can increase.
Scapula squeeze exercises
These exercises are designed to develop control over the shoulder blades by squeezing them back and holding them.
Patient Education
Learning proper posture is an important part of rehabilitation. For example, when your shoulders roll forward as you lean over a computer, the tendons in the front of the shoulder can become impinged. Your physical therapist will work with you to help improve your posture, and may suggest adjustments to your work station and work habits.
Functional Training
As your symptoms improve, your physical therapist will teach you how to correctly perform a range of functions using proper shoulder mechanics, such as lifting an object onto a shelf or throwing a ball. This training will help you return to pain-free function on the job, at home, and when playing sports.
References
[bg_collapse view=”button-orange” color=”#4a4949″ expand_text=”Show More” collapse_text=”Show Less” ]
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5729225/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3945046/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5441616/
- https://www.ncbi.nlm.nih.gov/pubmed/15866244
[/bg_collapse]

Visitor Rating: 5 Stars